We have begun a new series on the blog about PCOS, or Polycystic Ovarian Syndrome. This is an abnormal hormonal and metabolic condition that is common in women of size.
Today let's talk about the testing and diagnosis of it.
Previously we discussed the
definition and symptoms of PCOS, and how it often
presents in women.
In the future, we'll discuss its treatment, how it affects fertility, pregnancy, and breastfeeding, and its effects on menopause and aging.
But for now, let's talk about how to find out whether or not you have it, including what type of care providers to see, what type of tests are usually ordered and why, what they mean, and diagnostic debates.
Diagnostic Criteria for PCOS
PCOS is a somewhat controversial diagnosis. Unfortunately, this means that not everyone agrees on the best way to diagnose it. For example, 3 different organizations have come up with 3 slightly different criteria for diagnosis over the past 20+ years.
In 1990, the NIH came up with the following
criteria to diagnose PCOS:
- Clinical and/or biochemical hyperandrogenism
- Chronic anovulation
- Exclusion of related disorders
In 2003, the
Rotterdam criteria were developed. To be diagnosed via the Rotterdam criteria, a woman must have
two of the following three manifestations:
- Irregular or absent ovulation
- Elevated levels of androgenic hormones
- Enlarged ovaries containing at least 12 follicles each.
To make things even more confusing, the
Androgen Excess Society recently came up with its own criteria too:
- presence of hyperandrogenism (clinical and/or biochemical)
- ovarian dysfunction (oligo-anovulation and/or polycystic ovaries)
- exclusion of related disorders
Fortunately, all of these different criteria have some similarities. They are all basically looking for:
- evidence of disturbed menstrual cycles/ovulation, and
- evidence of elevated androgens (male hormones)
These seem to be the key items in deciding whether someone has PCOS or not. However, since these all occur on a wide spectrum of severity, the milder presentations of these symptoms can still make the diagnosis ambiguous at times.
Variations in Interpreting the Criteria
Some doctors are more strict in their interpretation of these criteria than others. For example, some doctors consider women to have PCOS only if they have few, if any, menstrual periods. Others consider any menstrual cycle longer than about 35-40 days to be abnormal and indicative of PCOS. Still others require 8 or fewer menstrual cycles per year (which translates to cycles of about 45+ days each).
Some doctors require that you demonstrate impaired fertility, and believe that any woman who has had children without fertility treatment could
not have PCOS. Others believe that some women can have spontaneous pregnancies yet still demonstrate other symptoms strongly enough that PCOS is likely.
Some doctors require lab work confirming that a woman has elevated androgen levels, while others will take physical symptoms of androgen excess (facial hair, thinning scalp hair, cystic acne) as enough proof of elevated androgens.
Ovarian follicles/cysts are now considered a particularly "soft" diagnostic requirement, since some women have cystic ovaries but no other symptoms of PCOS, while others clearly are symptomatic of PCOS yet do not have cystic ovaries. However, polycystic ovaries are a possible marker, so many providers still look for them, just not as "the" defining symptom of the syndrome.
The Rotterdam criteria is controversial because only 2 of the 3 criteria are needed for diagnosis, and "irregular" as well as "chronic" anovulation is considered. This opens up official diagnostic recognition to more borderline cases, such as:
...women with hyperandrogenism and polycystic ovaries but normal ovulatory function, and women with ovulatory dysfunction and polycystic ovaries but no clinical or biochemical evidence of hyperandrogenism (Azziz 2004, see references below).
In other words, it significantly widens the scope of who could be considered to have PCOS, while other criteria defines it more narrowly.
At this point, authorities are still debating the "best" criteria and who should and should not be considered to have PCOS. Diagnostic criteria are still evolving.
Testing for PCOS: An Overview
There is no simple test to measure conclusively whether or not someone has PCOS. Therefore, in order to try and diagnose PCOS, care providers usually:
- do a medical history to elicit menstual and fertility history
- do a physical exam to check for clinical evidence of symptoms
- do blood work to check various hormone levels
- do an ultrasound of the ovaries (not always done by every care provider)
PCOS tends to be a
diagnosis of exclusion, meaning that other conditions that might cause similar symptoms must be ruled out before one can conclude that PCOS is present. Among others, these
conditions might include:
Blood work in particular is helpful in ruling out these other conditions, since many present with similar symptoms to PCOS (hirsutism, mentrual irregularities, weight gain, etc.).
Getting Diagnosed: What Type of Care Provider?
A difficult question for many women is what type of provider to see when trying to decide whether or not they have PCOS. Unfortunately, there is no definitive answer to this question.
Women with PCOS have been diagnosed and treated by Family Doctors, GPs (General Practitioners), Internists, Midwives, OBs, Endocrinologists, and Reproductive Endocrinologists. Occasionally PCOS is caught by a Dermatologist or other specialist, but the patient is usually referred back to another specialty for further testing and treatment of non-skin symptoms.
Many women see their family doctor or GP (General Practitioner) for testing. The advantage of this is that the family doctor or GP tends to be less fat-phobic on average than specialists, and tend to listen better at appointments. However, not every family doctor or GP has very deep or thorough knowledge about PCOS and its proper testing and treatment.
Midwives and OBs are often the main source of diagnosis because PCOS problems usually reach critical levels around menstrual, fertility, gynecologic, or obstetric issues. Therefore, many midwives and OBs catch previously undiagnosed cases of PCOS when women come in for birth control advice, infertility care, maternity care, or with questions about skipped periods.
The advantage of midwives is that they are generally more size-friendly than doctors, have training in gynecological issues, listen better, and take more time with you in appointments. However, not all are well-versed in such a specialized condition as PCOS.
Because of fertility issues, many women get their diagnosis of PCOS from OBs. And while many OBs are reasonably knowledgeable about PCOS, there's still a lot of misinformation about it even in the obstetric community. Furthermore, there's a lot of fat-phobia in medical training and in obstetrics in particular; this means that some OBs have a hard time treating a woman of size with compassion and objectivity.
Because PCOS is a hormonal and metabolic issue at heart, endocrinologists
should be the go-to specialty for diagnosis of PCOS. They tend to be more well-versed in PCOS than the average care provider (especially the Reproductive Endocrinologist sub-specialty), and they have an intimate knowledge of the pros and cons of various tests and treatments for PCOS. Unfortunately, endocrinologists have an extremely well-deserved reputation for fat-phobia, and that can make it hard for fat people to get good care from them.
So what do you do?
Making a Decision
When deciding which type of care provider to see about testing for PCOS, there are a couple of important questions to ask. First, how important is it to you to avoid even the merest whiff of size bias; second, are you in a rush to have a child; and third, what do you know about the size-friendliness of various providers in your area?
If you can stand the possibility of size bias, an endocrinologist really is best place to start your diagnostic journey. They are the ones with the specialized knowledge about PCOS, the ones who know which tests to order to rule out other possibilities, and they are more inclined to treat PCOS with insulin-sensitizing agents instead of just birth control pills, which may be important for long-term health.
On the other hand, if you already have a good relationship with an OB, that can be a decent place to start. Just keep good track of the tests ordered so you can make sure the right tests are being used and the right follow-ups are being done.
If size-friendliness is really important to you and you don't know the weight-neutrality status of any local providers, the midwife or the family practice doctor may be a good place to start instead. Of course, title alone does not guarantee size-friendliness, but generally speaking you'll probably encounter less fat-phobia on average in these two groups.
If fertility is an issue for you or you are wanting to get started on having a child ASAP, go straight to a Reproductive Endocrinologist. They are
the specialists in PCOS and tend to get you into treatment (and hopefully, fertile enough for pregnancy) a lot sooner than the other specialties.
Of course, the best option is
finding a size-friendly/weight-neutral provider, whatever their title. Although it's certainly not comprehensive for all locations, remember the
Fat-Friendly Health Professionals List, which has peer-to-peer recommendations for size-friendly providers in the USA, and this
similar list for Australia.
Preparing for an Diagnostic Appointment
A little prep work can go a long way towards making your diagnostic appointment faster and easier.
First, write down a
list of your symptoms so you don't forget to mention anything. Include both obvious PCOS symptoms and those that may not have anything to do with PCOS, since things like headaches and vision problems can sometimes be associated with conditions that can mimic PCOS (like a benign pituitary tumor). Have your list on a separate sheet of paper so you can just give it to the care provider, which will speed up the appointment considerably.
Also
document your cycles for as long as you can ─ their length, regularity, and severity ─ and any concerns you have about them (length, heaviness, spotting, severe cramps, etc.) Make an extra copy of this for the care provider.
If you have been doing
fertility charting, bring those charts along to document whether/when you ovulate, how long you bleed, etc. Some providers will take these seriously, some will not, but they are definitely worth doing because they are a very powerful tool for figuring out what's going on. Be sure to keep copies for yourself for future reference. (See the
website or the book,
Taking Charge of Your Fertility, for more information on how to do fertility charting.)
A
list of your current medications (if any) and dosages would also be important, since medications can sometimes affect lab results or have side effects that mimic PCOS symptoms.
It's a good idea to have a
list of questions you want to ask. You may not always have time to ask everything at the first appointment because care providers are usually on very strict schedules, but it can help you prioritize your questions so the most important ones get asked first, and help you remember your other questions for follow-up appointments.
Before your appointment, be sure to gather all your pertinent
medical records together. If you have records of previous labs or other tests, have these sent ahead of time to the new provider, or bring copies of them yourself. This can save a lot of time and duplication. Some tests will need to be repeated, regardless, but it's useful to have a record of your results over time. Many people create a simple spread sheet, documenting pertinent tests over time, which can be useful in tracking any fluctuations in your condition.
The
timing of your appointment may be important. If you want the care provider to order hormonal tests, the best time for such tests is shortly after your period. Avoid the time around mid-cycle or ovulation, as this can affect hormone levels.
Make your appointment for first thing in the morning, while you are in a
fasting state. Certain tests need to have a 12-hour fast before doing the test. If you arrive fasting, you can do all these tests on the same day and won't have to come back to do them another day.
If you are concerned about finding a
size-friendly provider, call or write a letter ahead of time that asks if the provider can provide
size-friendly care, and whether they are able to respect your decision to avoid focusing on weight loss. Or bring an advocate with you, someone who can take notes and help you speak up for yourself if the provider starts focusing only on weight. (Obviously, this person should be someone you would be comfortable with hearing a discussion of intimate topics like menstrual periods, birth control, etc., and someone who shares your beliefs about size acceptance.)
Really
thinking through your appointment ahead of time and even rehearsing what you are going to say can be very helpful if you have are nervous about the appointment or have had bad experiences with care providers in the past. Don't forget that YOU are the employer and the care provider is your employee; you always have the right to decline tests or treatment you do not want, or to terminate the relationship if needed.
The Diagnostic Appointment
At your diagnostic appointment, your care provider should take a
medical history, do a
physical exam, and start the
blood work needed for diagnosis.
More than one appointment may be needed to do do follow-up lab work. Afterwards, there should be an appointment to discuss the results of testing and to develop a treatment plan, if needed.
Medical History
The first thing a care provider should do when trying to diagnose PCOS is to take a medical history This exam should look something like
this:
A health care professional...will ask questions about your menstrual history, including how old you were when you started your period, how long your cycles are, how much time passes between cycles, and how much you bleed in a cycle. Your health care provider will also ask about your reproductive history, including any pregnancies, miscarriages, or abortions you have had, and birth control methods you are using or have used in the past. He or she will also ask about menstrual irregularities in other members of your family.
In addition, the woman should be asked about the presence of other symptoms, like hirsutism, acne, scalp hair loss, sebaceous cysts, or nipple discharge. Although sometimes neglected, a weight history should be taken as well, looking for episodes of unexplained weight gain, difficulty losing weight, etc.
Family medical history should also be asked about. There is a strong genetic predisposition in some families towards PCOS, with frequent history of irregular menstrual cycles, hirsutism, diabetes, hypertension, or infertility among females, and premature balding and the metabolic syndrome among males. A history of any of these in your family would increase the suspicion index for PCOS.
Finally, the care provider should review any medications you have been on. Although rare, some medications can cause PCOS-like symptoms to occur (for example, chronic use of corticosteroids, or anti-seizure medications like Depakote). In addition, certain medications (like birth control pills) can alter lab results on certain tests (like SHBG levels).
Physical Exam
Next, a physical exam should be done. The care provider will look for hirsutism (excess facial or body hair, especially along the midline of your body), acanthosis nigricans (dark, velvety patches of skin on the thighs, armpits, or back of the neck), skin tags, central obesity, etc. Be sure to tell your care provider about any symptoms you have, including thinning hair etc., so they are sure to take it into account.
Height, weight, and blood pressure will be checked. This is one occasion when it is appropriate for a woman to be weighed, if only to document "obesity" as a possible symptom ─ but preferably in a weight-neutral and non-judgmental manner. Blood pressure should be checked using an appropriately-sized cuff (a too-small cuff will falsely elevate blood pressure).
A pelvic exam is also common, with care providers checking to see if your ovaries seem enlarged or swollen. They will also check to see if your genitalia look normal (an unusual appearance can indicate adrenal hyperplasia) and whether there are any pelvic masses.
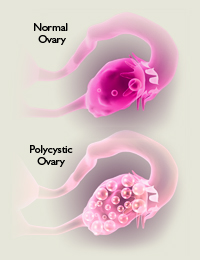
Some doctors order an ultrasound to check for the presence of ovarian cysts. Because of hormonal imbalances, women with PCOS often have difficulty finishing ovulation. This half-finished ovulation causes many small cysts all over the ovaries, giving it a characteristic "string of pearls" appearance, as in the picture at the top of this post. One diagnostic criteria for polycystic ovaries is 12 or more cysts of 2-9 mm size (but some practices have different guidelines).
Remember, even if the ovaries do appear normal, the absence of ovarian cysts does not mean that you don’t have PCOS. Not everyone with PCOS has ovarian cysts.
Bloodwork
Multiple blood tests are usually run. Lab work may include some or all of the following:
- Follicle Stimulating Hormone (FSH)
- Luteinizing Hormone (LH)
- Total or Free testosterone
- Other androgenic hormones like Androstenedione
- DHEA-S (dehydroepiandrosterone sulfate)
- Sex Hormone Binding Globulin (SHBG)
- Cortisol (and/or other adrenal hormones)
- Prolactin
- TSH (Thyroid Stimulating Hormone)
- Free T3 and free T4 levels
- Thyroid antibody tests
- Anti-Mullerian Hormone (AMH)
- 17-hydroxyprogesterone (17OH-progesterone)
In addition, most doctors will order labs for standard measures of health, like cholesterol, triglycerides, blood sugar, etc. Some will do these in conjunction with PCOS bloodwork; some will wait and only do these after PCOS has been confirmed.
Some providers add liver function tests to be sure you are not experiencing Non-Alcoholic Fatty Liver Disease (NAFLD). Others may also check levels of certain nutrients, like Vitamin D or iron, because these are often abnormal in women with PCOS.
Be aware that certain tests (like LH and FSH) need to be taken on certain days of your cycle in order to be interpreted correctly. Unfortunately, not all doctors are aware of this, and may test on inappropriate days. If you have been told you do not have PCOS but were tested without regard to day of your cycle, these tests should be repeated before ruling out PCOS.
Interpreting Results
Results on these tests can be confusing and it's very important that you get help interpreting them. Remember to ask for
exact results, not just whether your levels are "normal" or "abnormal," because borderline results may be meaningful in some contexts.
It's best to ask for a copy of all lab results; this is your information and you have every right to it. That way you can take those results to another provider if needed, and you can also track your results over time.
The following are a few test results that seem common in women with PCOS, according to various
resources online. However, tests results are always subject to interpretation and our understanding of these things changes over time, so be sure to discuss your results with a healthcare professional.
- A high testosterone level is common with PCOS but is not an absolute requirement for it. Very high levels may indicate an adrenal tumor instead
- The DHEA-S level is often mildly elevated in PCOS, but this could also indicate an adrenal issue instead of PCOS (or in addition to it)
- Androstenedione is often somewhat elevated
- Sex Hormone Binding Globulin (SHBG) is usually low in PCOS, and seems to be associated with insulin resistance and/or hypothyroidism
- A high prolactin level probably indicates hyperprolactinemia; some women with PCOS have mildly elevated prolactin levels, but very high levels are usually due to hyperprolactinemia
- FSH levels are usually low to normal, but LH levels are often high. A level of 2:1 or more in the LH:FSH ratio is usually considered diagnostic for PCOS
- Lipid profiles are often abnormal; a common pattern is borderline to high LDL, low HDL, and high triglycerides
- TSH is often borderline high but not quite high enough for diagnosis under the criteria some doctors use. However, some sources believe that any TSH over 2 or so should be treated
Blood Sugar and Insulin Testing
Blood sugar tests are a standard part of testing because of the high rate of diabetes associated with PCOS. However, there are several ways to test this.
Some providers use fasting glucose only, but some
resources feel strongly that this misses some cases of diabetes. They think PCOS women should be tested using a 2-hour Oral Glucose Tolerance Test (OGTT) instead. However, many women with PCOS have a tendency towards reactive hypoglycemia (unstable blood sugar due to strong insulin surges) and find the OGTT makes them feel quite ill. Therefore which test should be used is a judgment call.
Checking insulin levels is
controversial. Just about everyone agrees that insulin resistance is a major issue in PCOS, but how best to measure it is debated. The gold standard test is hyperinsulinemic/euglycemic clamp testing, but this is usually too cumbersome and expensive for anything but research studies.
Some doctors test fasting insulin levels, because this is an easy lab draw. Anything over 20 μU/mL is considered abnormal, but critics point out that the "normal" range for this is quite wide, and contend that levels much lower than 20 show insulin issues. Some prefer to use a fasting glucose/insulin ratio instead, looking for a ratio of less than 4.5, but critics point out that this ratio has not been validated using clamp techniques.
One technique that has been validated by clamp techniques is Homeostatic Model Assessment (HOMA) testing, which takes fasting glucose and fasting insulin and divides them by a constant. However, this (like all of the fasting tests) is criticized as missing many cases of insulin resistance, because many PCOS women have relatively normal levels while fasting but abnormal insulin and glucose levels in response to food intake. Therefore, many doctors prefer to order a 2-hour post-prandial insulin test or OGTT, where your insulin response is tested after eating food or the standardized glucose liquid.
Here is what one provider
wrote about testing insulin levels. Other providers may find these criteria too liberal:
Fasting insulin is often elevated in PCOS. Some doctors don't order this test because the normal range (0-20) is so wide. However, we find that results greater than 9 indicate insulin resistance...Some doctors may also order a 2-hour post-prandial insulin test, along with a 2-hour post-prandial glucose test. For the post-prandial insulin, results over 25 or 30 may indicate insulin resistance.
On the other hand, some doctors don't test insulin levels at all, either because they believe that insulin levels are not as relevant as hormonal levels, or because they don't believe that insulin testing is that meaningful. They may go by clinical signs of insulin resistance instead (acanthosis nigricans, skin tags, abdominal obesity, etc.).
Other Tests
As previously noted, doctors used to do a vaginal ultrasound to see if the ovaries had a "string of pearls" look, studded with cysts. Now however, many providers do not consider cystic ovaries to be a very good measure of PCOS. Some will test for it, some will not.
Providers are becoming more aware that sleep apnea is fairly
common among women with PCOS, so some have added sleep testing to the list of additional tests ordered after someone is diagnosed with PCOS. Some
research suggests that testing for sleep apnea is underutilized in women with PCOS and should be expanded, especially for those with more
severe insulin resistance/glucose intolerance.
If your preliminary labs or symptoms suggest that you may have non-classical congenital adrenal hyperplasia instead of PCOS, your doctor may want to order additional labs, including an ACTH (adrenocorticotropic hormone) stimulation test.
If your providers suspect Cushing's syndrome, they may order a 24-hour urine test for free cortisol, or suggest an overnight dexamethasone suppression test.
If you are someone who has no or very few menstrual cycles (less than 6 per year), care providers may also recommend an endometrial biopsy. Because of a hormonal imbalance, many women with PCOS do not completely slough off the endometrial lining that has built up during a cycle. Over time, this endometrial lining can build up ("endometrial hyperplasia") and cause problems.
The risk for endometrial cancer is signficantly higher in women who do not have at least six periods per year, so if you have missed a lot of periods, it's
very important that you get checked periodically for this.
Changes in Diagnosis Protocols Over The Years
The protocol for diagnosing PCOS has changed over the years and remains controversial.
As noted, some doctors insist on an ultrasound of the ovaries, while others consider that outdated or unnecessary. Some demand biochemical evidence of abnormal hormone levels (i.e., abnormalities on lab tests), while others are content to rely on physical manifestations alone. Some run elaborate blood tests to rule out a wide variety of other possible conditions, while others are willing to move to a trial of meds and/or lifestyle more quickly based on symptoms alone. Much depends on the care provider you see.
Doctors used to look for a specific imbalance of hormones ─ specifically a ratio of luteinizing hormone (LH) to follicle-stimulating hormone (FSH) of more than 3:1. Some doctors still look for elevated LH levels (although not necessarily a 3:1 ratio anymore), while others do not test these levels at all.
Some doctors believe that insulin resistance (either through an insulin receptor defect or through post-receptor signaling) is the base cause of PCOS, while others believe that while common, not every woman with PCOS actually demonstrates insulin resistance. So while some doctors place a strong emphasis on insulin levels in PCOS, others don't.
A recent addition to testing protocols seems to be "
anti-mullerian" hormone levels:
Anti Mullerian Hormone (AMH) or Mullerian Inhibiting Substance is a special protein released by cells that are involved with the growth of an egg follicle each month. AMH levels correlate with the number of antral follicles found on the ovary each month; the higher the antral follicle count, the higher the AMH levels. Because women with PCOS typically have high numbers of antral follicles, high AMH levels are often seen as well.
Apparently some doctors are considering AMH a classic marker for the disease now and want this tested; others do not routinely use it.
Obviously, diagnosing PCOS is an evolving science. Tests that were routine 10-15 years ago are not always considered necessary now, and new tests have emerged that didn't exist previously. This is why it's important to keep up on the latest testing protocols and the pros and cons of each test.
Conclusion
It should be apparent that diagnosing PCOS is not an easy task. Different protocols for testing and diagnosis exist, standards change over time, and the highly variable nature of PCOS makes diagnosis less than clear at times. A great deal is left up to the individual judgment of the care provider.
Therefore, it is not uncommon for women to hear different results from different doctors, with one saying she doesn't have PCOS, and another saying she does. Some women with PCOS go for
years before they are diagnosed, even with obvious symptoms. Subtle cases may take even longer.
Persistence is very important in trying to figure out whether or not you have PCOS. Don't give up easily, and be prepared to see more than one care provider when trying to find answers. Most women go through
multiple care providers and tests before they are able to definitively determine that they do or don't have PCOS.
Sometimes a person's results may be "borderline normal" and that can still be significant, especially if there is a cluster of similarly "borderline" results on other tests. As Dr. Samuel Thatcher says in
PolyCystic Ovarian Syndrome: The Hidden Epidemic:
Virtually all patients with PCOS will have at least some subtle laboratory abnormalities. The reported results may be on the upper limits of the normal range, showing only a tendency rather than a discrete abnormality. Often a pattern will emerge only after considering a group of tests together, rather than as a result of a single test value.
Furthermore, don't accept a care provider's pronouncement about your PCOS status without looking at your own lab results, comparing them to what is considered "normal," and researching the results online. Because knowledge about PCOS is evolving, not all providers are "up" on the best ways to test it or changes in diagnostic protocols. Furthermore, anti-fat bias can lead some to dismiss or explain away results that clearly merit a second look. It's important to double-check their work.
Remember that diagnosis can be a judgment call at times, so you should plan to be
actively involved in the process. Don't be a passive recipient of care; get copies of all of your lab results, create a spread sheet to track them over time, research PCOS online from a variety of sources, ask lots of questions, and don't be afraid to switch care providers if you don't feel your questions and concerns are being addressed adequately.
Don't forget that there is a spectrum of PCOS severity. Even if you do not officially "qualify" as having PCOS, it may still be something you should learn about because some cases are too "mild" for official diagnosis but may still benefit from treatment or careful monitoring of health indices.
Finally, if you don't have PCOS, don't be afraid to push for further testing to explain your symptoms. PCOS is not the only thing that can be wrong in people of size, and treatment for rarer conditions like Cushing's Syndrome or adrenal tumors can make a tremendous difference in your health. Explore
all the possibilities.
Diagnosing PCOS is not an exact science, but finding answers can be critical for your long-term health status.
References
Finding Size-Friendly Care Providers
General Resources for PCOS Support
General Information about PCOS
Book Resources
- PolyCystic Ovarian Syndrome: The Hidden Epidemic - Samuel S. Thatcher MD, PhD
- Androgen Disorders in Women: The Most Neglected Hormone Problem - Theresa Cheung
- Taking Charge of Your Fertility - Toni Weschler; www.tcoyf.com
Information about PCOS Testing and Diagnosis
Interpreting Lab Results - What is Normal?
Specific PCOS Diagnosis Studies
Reprod Biomed Online. 2004 Jun;8(6):644-8.
PCOS: a diagnostic challenge. Azziz R. PMID:
15169578
"Useful research and diagnostic criteria for PCOS arose from a conference in 1990, whereby PCOS could be defined by: (i) clinical and/or biochemical hyperandrogenism, (ii) chronic anovulation, and (iii) exclusion of related disorders. The presence of "polycystic ovaries" was not included in this definition, which created significant concern since many women with PCOS have polycystic ovaries on ultrasound, and conversely women with this ovarian morphology have a higher prevalence of androgen excess and insulin resistance. More recently, at an expert meeting in 2003 in Rotterdam, it was recommended that PCOS be defined when at least two of the following three features were present, after exclusion of other aetiologies: (i) oligo- or anovulation, (ii) clinical and/or biochemical hyperandrogenism, or (iii) polycystic ovaries. These newer criteria effectively create additional phenotypes of PCOS (e.g. women with hyperandrogenism and polycystic ovaries but normal ovulatory function, and women with ovulatory dysfunction and polycystic ovaries but no clinical or biochemical evidence of hyperandrogenism). It remains to be demonstrated whether these phenotypes actually represent patients with PCOS. Nonetheless, the trend towards the use of uniform diagnostic criteria in studies of PCOS will increase the comparability and potentially the value of published research."
Fertil Steril. 2009 Feb;91(2):456-88. Epub 2008 Oct 23.
The Androgen Excess and PCOS Society criteria for the polycystic ovary syndrome: the complete task force report. Azziz R, Carmina E, Dewailly D, Diamanti-Kandarakis E, Escobar-Morreale HF, Futterweit W, Janssen OE, Legro RS, Norman RJ, Taylor AE, Witchel SF; Task Force on the Phenotype of the Polycystic Ovary Syndrome of The Androgen Excess and PCOS Society. PMID:
18950759
"Based on the available data, it is the view of the AE-PCOS Society Task Force that PCOS should be defined by the presence of hyperandrogenism (clinical and/or biochemical), ovarian dysfunction (oligo-anovulation and/or polycystic ovaries), and the exclusion of related disorders. However, a minority considered the possibility that there may be forms of PCOS without overt evidence of hyperandrogenism, but recognized that more data are required before validating this supposition. Finally, the Task Force recognized and fully expects that the definition of this syndrome will evolve over time to incorporate new research findings."
"Development of a questionnaire to help diagnose PCOS. "A history of infrequent menses, hirsutism, obesity, and acne were strongly predictive of a diagnosis of PCOS, whereas a history of failed pregnancy attempts was not useful. A history of nipple discharge outside of pregnancy strongly predicted no diagnosis of PCOS. We constructed a 4-item questionnaire for use in diagnosis of PCOS; the questionnaire yielded a sensitivity of 85% and a specificity of 85% on multivariate logistic regression and a sensitivity of 77% and a specificity of 94% using the 4-item questionnaire."
Hum Reprod. 2004 Jan;19(1):41-7.
Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome (PCOS). Rotterdam ESHRE/ASRM-Sponsored PCOS consensus workshop group. PMID:
14688154
"Since the 1990 NIH-sponsored conference on polycystic ovary syndrome (PCOS), it has become appreciated that the syndrome encompasses a broader spectrum of signs and symptoms of ovarian dysfunction than those defined by the original diagnostic criteria. The 2003 Rotterdam consensus workshop concluded that PCOS is a syndrome of ovarian dysfunction along with the cardinal features hyperandrogenism and polycystic ovary (PCO) morphology. PCOS remains a syndrome and, as such, no single diagnostic criterion (such as hyperandrogenism or PCO) is sufficient for clinical diagnosis. Its clinical manifestations may include: menstrual irregularities, signs of androgen excess, and obesity. Insulin resistance and elevated serum LH levels are also common features in PCOS. PCOS is associated with an increased risk of type 2 diabetes and cardiovascular events."
Clin Endocrinol (Oxf). 2005 Mar;62(3):289-95.
Polycystic ovarian syndrome: marked differences between endocrinologists and gynaecologistsin diagnosis and management. Cussons AJ et al. PMID:
15730409
"...A mailed questionnaire containing a hypothetical patient's case history with varying presentations--oligomenorrhoea, hirsutism, infertility and obesity--was sent to Australian clinical endocrinologists and gynaecologists in teaching hospitals and private practice...Endocrinologists regarded androgenization (81%) and menstrual irregularity (70%) as essential diagnostic criteria, whereas gynaecologists required polycystic ovaries (61%), androgenization (59%), menstrual irregularity (47%) and an elevated LH/FSH ratio (47%) (all P-values less than 0.001). In investigation, gynaecologists were more likely to request ovarian ultrasound (91%vs. 44%, P less than 0.001) and endocrinologists more likely to measure adrenal androgens (80% vs. 58%, P less than 0.001) and lipids (67%vs. 34%, P less than 0.001). Gynaecologists were less likely to assess glucose homeostasis but more likely to use a glucose tolerance test to do so. Diet and exercise were chosen by most respondents as first-line treatment for all presentations. However, endocrinologists were more likely to use insulin sensitizers, particularly metformin, for these indications. In particular, for infertility, endocrinologists favoured metformin treatment whereas gynaecologists recommended clomiphene. CONCLUSIONS: There is a lack of consensus between endocrinologists and gynaecologists in the definition, diagnosis and treatment of PCOS. As a consequence, women may receive a different diagnosis or treatment depending on the type of specialist consulted.
Clin Endocrinol (Oxf). 2008 Jul;69(1):52-60.
The evaluation of metabolic parameters and insulin sensitivity for a more robust diagnosis of thepolycystic ovary syndrome. Amato MC, et al. PMID:
18034780
PCOS diagnostic criteria [National Institute of Health (NIH), Rotterdam Consensus (ROT), Androgen Excess Society (AES)] are unanimous recognized. We aimed to assess in women with suspected PCOS whether the application of the three diagnostic criteria differently characterizes the metabolic profile and insulin sensitivity. Two hundred and four women with suspected PCOS in comparison to a group of normal, age-matched Sicilian women (N = 34) without signs of metabolic syndrome...The prevalence of PCOS was 51% according to NIH, 83% to ROT and 70.6% to AES, and only 100 patients were qualified simultaneously under these three criteria.